During 2025, as I continued to work with our Document Services group on finding ways to improve the experience of documents, it became increasingly clear that duplicate documents were a growing burden across our client base. For staff, they created document management problem as repeat documents piled up and required extra triage. For clinicians, they created a findability problem in the patient chart, increasing patient safety risk by making it unclear which document to trust.
Even our recent survey data had pointed out this problem of duplicates
This pain was especially visible in a high volume of issues coming from newly onboarded clients, who were frequently reporting duplicate documents in the chart. Leadership wanted us to investigate this problem so we could develop a strategy for addressing duplicates heading into 2026.
❔THE QUESTION
How might we lessen the burden of duplicate documents coming into the system?
🔍 Discover
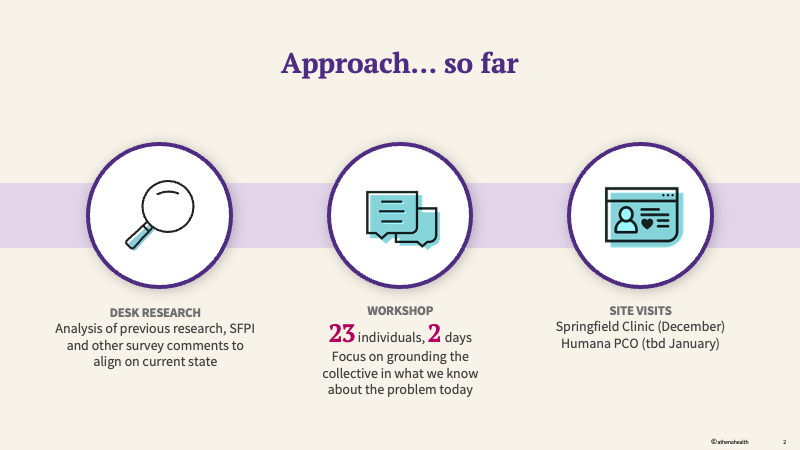
Because we already had a solid knowledge-base pulled together from our previous research into documents, it was easy for me to break things out into a solid set of “dupe cases,” each of which required a slightly different means of dealing with them. Within a compressed timeframe, I was able to pull together the basic framing of the problem space, which we used to organize a workshop across all the teams that owned different aspects of the incoming document pipeline - including Fax, DIRECT, and Interfaces.
Our overall plan for the initiative laid the ground work for the plan we had to create
During the workshop, we established that typical, tech-driven de-duplication approaches rely on “exact matches” in the content. These approaches were not effective in an environment where:
the same information comes over though different channels and even in different formats, such as CCDA and fax
senders may send multiple copies of the same information to different providers, or send repeat requests of the same information on different days until they get a response
the system “splits up” the content of a document into multiple pieces when it comes in, creating a disconnected experience.
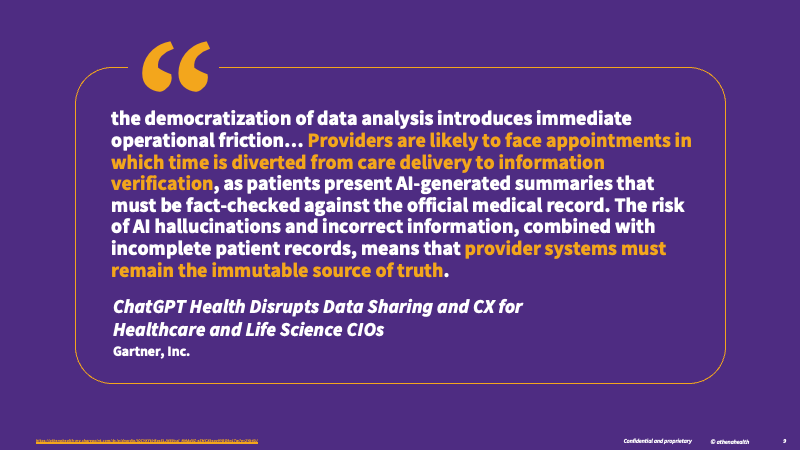
These problems have been exacerbated by a healthcare landscape increasingly focused on sending information across multiple interoperable channels and leaning on AI-generated summaries to provide relief against cognitive overload.
This quote from a recent Gartner report explained the situation well.
Following the workshop, I organized a site visit for myself and 6 other tech and product leaders to one of our larger clients, who had been dealing with this problem acutely. During the site visit, we witnessed first-hand the pain that these duplicates create across a variety of workflows - from prescription refills to imaging and diagnostic results and more.
📖 Define
Through the research, we were able to identify six main categories of duplicates and how they vary across document types, sources, and workflows. Each category had its own implications for:
how the content showed up in the system
the patterns that might govern why someone would consider it a duplicate
what sources (fax, Direct, interface) the content is likely to come from
how we could address the duplicate without risking patient safety or workflow efficiency
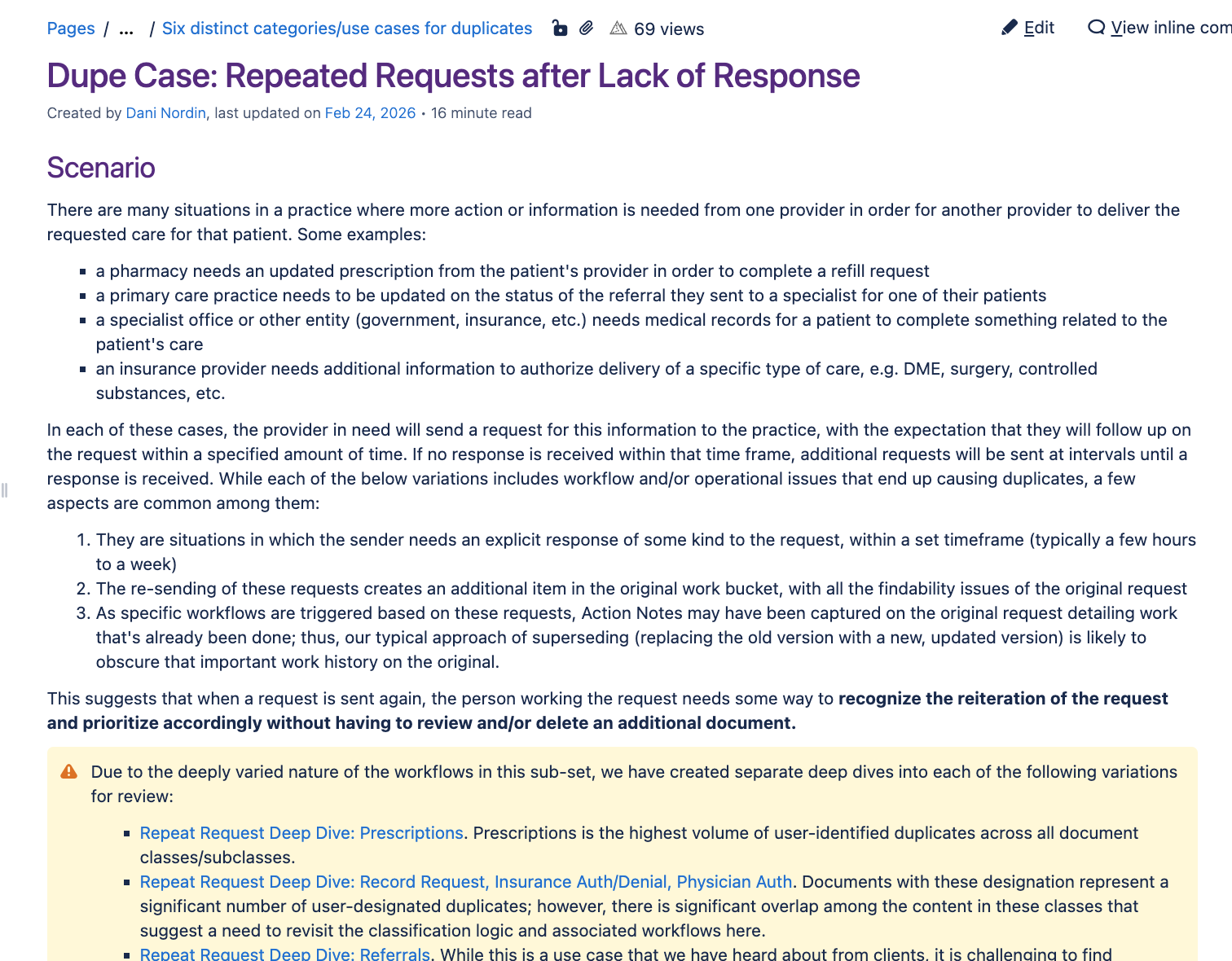
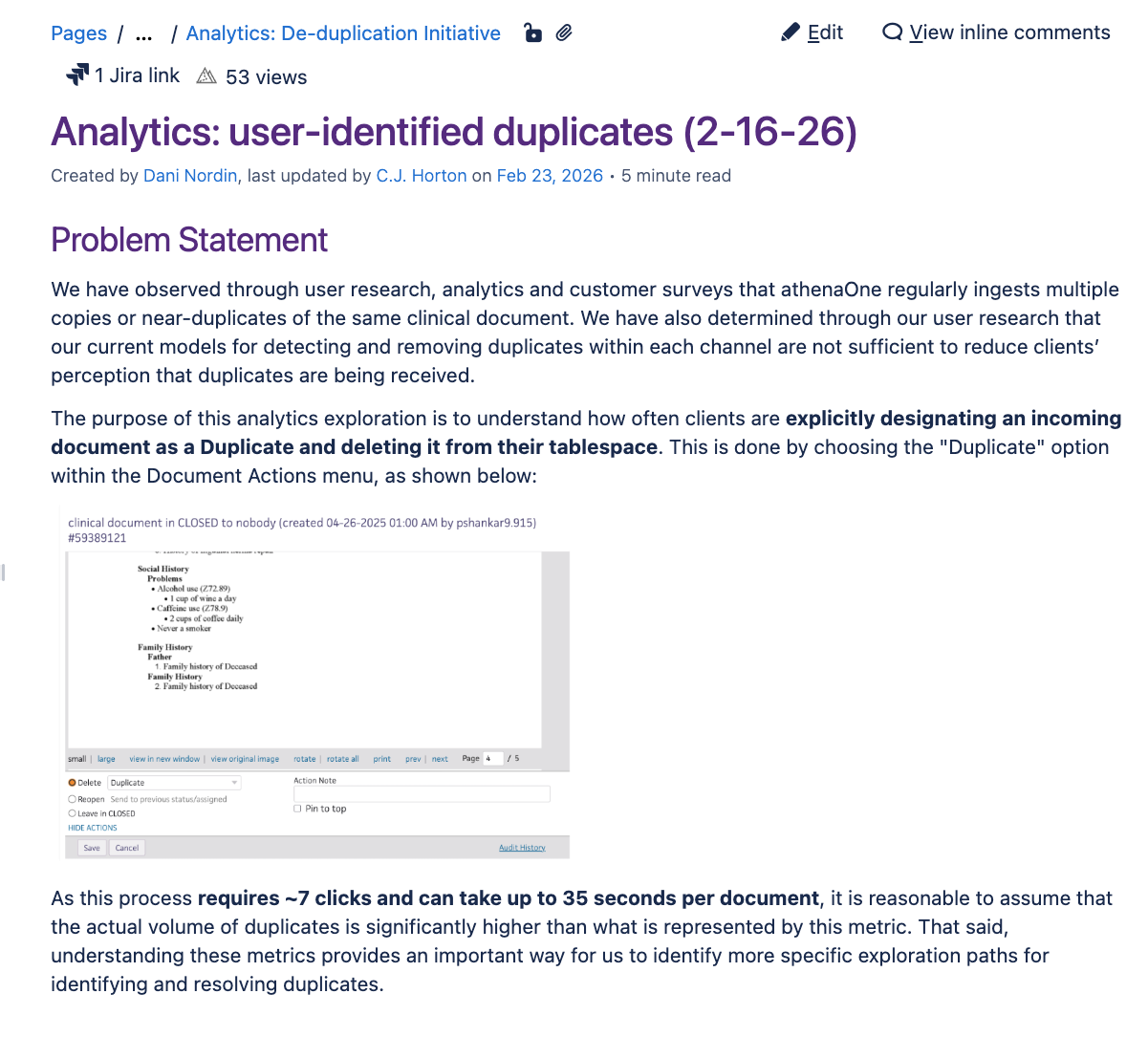
To flesh these out, I create a series of “dupe cases” that dove deep into each of these categories. Each case included examples of how these documents show up in workflow, along with screenshots of the distinctions we might see in the content that shows it’s a duplicate even if it’s coming from different sources. They also included a list of the potential data elements we could compare to determine whether it’s a duplicate, since one of the most important channels we were comparing was Fax - which doesn’t have structured information such as an accessionID to compare against.
Our Dupe Cases helped quantify and contextualize each type of duplicate users were experiencing.
Throughout the process, I kept a tight partnership with Data Science. The content analysis I did with real examples helped contextualize what were seeing in analytics data, which ultimately helped the Product team determine which cases needed to be prioritized.
We combined user research with analytics and content analysis to inform our prioritization.
📐 Align
We approached this work as cross-zone and cross-division intentionally, because documents enter the system through multiple sources and workflows. Our early research quickly surfaced a key dynamic that was exacerbating the problem: the same information was often arriving through different channels, creating overlapping artifacts that were difficult for staff to manage and for clinicians to trust.
A bold problem statement grounded in user research helped us set the tone for the initiative across functions and subdivisions
To align on the problem space and pressure-test our early hypotheses, I facilitated a workshop with 15+ stakeholders across Platform and multiple Clinicals zones, bringing together the teams responsible for different parts of the incoming document pipeline. I then organized a cross-division site visit so product and technical leaders could see the impact of duplicates in real workflows and develop a shared understanding of what “duplicate” means in context.
“Howdy! I hear you are facilitating some awesome site visits. Both [colleagues] were bursting at the seams when I saw them in Boston this week. It made me so happy to see them ignited with curiosity!” - Exec Director Design, Platform
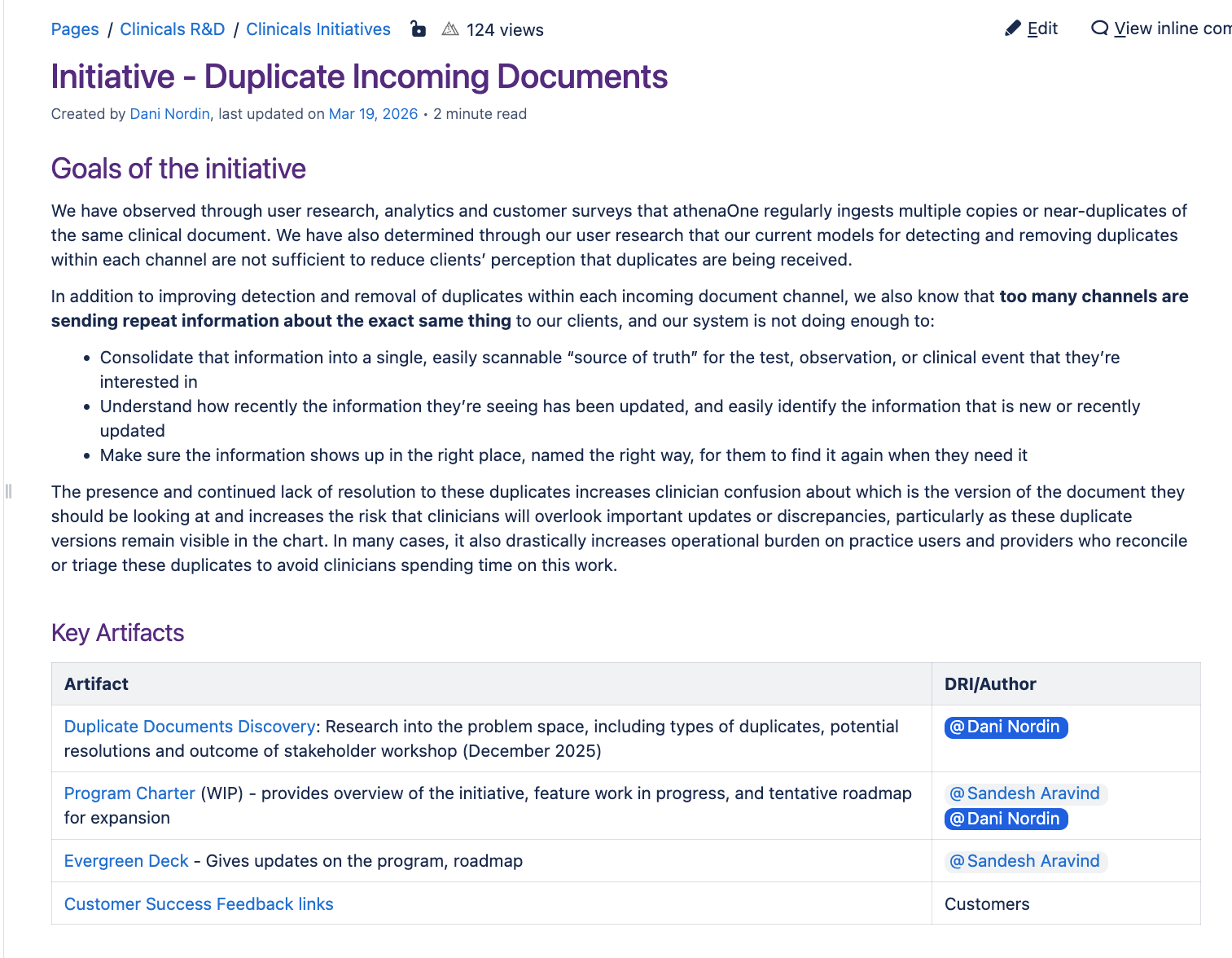
As with most of my projects, I documented this information for the group in a shared Confluence space that included all of the research artifacts, including extensive deep dives on the dupe cases.
By organizing the research in a shared Confluence space, our insights can keep informing strategy well into the future.
After the initial wave of research, the team and I stayed close with the cross-division partners to collaborate on shared roadmaps and keep knowledge flowing between teams, including sharing the research artifacts so each group could move forward with a consistent framing.
In parallel, I partnered with a Platform team to reimagine how Direct Messages could be structured in a way that lets attachments stay in the context of the message, improving findability and supporting clearer interpretation of what clinicians are seeing. This work not only helped us move forward on one of our dupe cases, the way we pressure-tested the use case helped the Platform team I was working improve their conversations with a key Clinicals zone to move forward a related but separate initiative:
“I’m hoping this [Hackathon work] opens a lot of doors to move things forward.” - Senior Manager Product, Platform
✅ Outcome
This work helped the cross-division teams align on some concrete use cases to start with, and prioritization is already underway. It also sparked several tangential threads that teams have already begun picking up. More broadly, the findings have informed multiple efforts across the business—including how we think about and approach CCDAs, results, and prescriptions—and each team is now developing a comprehensive roadmap that will span the next couple of years.
“I want to take a moment to thank you for your thoughtful leadership of the ‘duplicate document’ initiative on such short notice… Your commitment to and advocacy for our customers/users is commendable and important as we evaluate our options going forward. I look forward to building on the foundation we placed as we move into 2026.” - Exec Director Product, Clinicals